
VO2 max is the gold standard measure of cardiorespiratory fitness and has been hailed as a top predictor of longevity, but do you need a formal test to know yours? We unpack the evidence on VO2 max measurement with cardiopulmonary exercise testing, VO2 max estimation with wearables, and how they apply to your health.
__________________________________________________________________________
I’ve seen a lot of different takes on VO2 max lately. Some say it's the single strongest predictor of how long you'll live. Others argue that simpler measures of cardiorespiratory fitness are just as useful, and we should stop putting VO2 max on a pedestal. Two concerns keep coming up:
- In most studies linking fitness to mortality, VO2 max wasn't actually measured directly (which requires breathing into a mask during exercise). Instead, it was estimated from simpler exercise tests, or from equations that don't use exercise at all.
- A lot of people now rely on VO2 max numbers from their wearables (think Apple Watch, Garmin, Whoop), but there are questions about how accurate those numbers are.
Because proactive health care is our mission at NiaHealth, I went deep into the literature to make sure our recommendations around cardiorespiratory fitness and VO2 max testing line up with the best evidence. I also had a personal motive: I've never had a formal VO2 max test, instead relying on my Garmin fenix 7. And, well, let’s say that the estimate my wearable gives me feels like a bit of a vanity stat. I wanted to know: do I actually need a formal test to understand my current fitness and future health risk?
This evidence review took a lot longer than I expected. Every time I pulled on a thread, it led to another one. I think I've finally unravelled the sweater, and now it’s time to share what I found.
So: is VO2 max the be-all and end-all of longevity prediction? Should we abandon it for simpler measurements? And can we trust the number our wearables give us? Like everything in health, the answers are nuanced.
Let's start with some definitions.
What is cardiorespiratory fitness?
Cardiorespiratory fitness — usually shortened to CRF — is your body's ability to deliver oxygen to your working muscles during physical activity. More technically, it's "the integrated ability of the circulatory and respiratory systems to supply oxygen to skeletal muscle mitochondria for the energy production needed during physical activity" 1.
CRF is usually expressed one of two ways:
- VO2 max — the maximum amount of oxygen your body can use during intense exercise. The units are in millilitres of oxygen per kilogram of body weight per minute (mL O₂/kg/min).
- Maximum METs — the maximum amount of energy your body can produce during intense exercise, expressed as a multiple of how much energy you burn at rest.
Both measures tell us roughly the same thing. (More on this in the next section.) The key idea is that fitter people can sustain higher levels of effort–represented as higher VO2 max and METs–which means their hearts, lungs, blood vessels, and muscles are all working well together.
Quick note on VO2 max vs. VO2 peak You may see both terms used. VO2 max is the highest oxygen uptake your body is actually capable of (the true ceiling). VO2 peak is the highest oxygen uptake you reached during a specific test — which may or may not have been your true maximum. Some results from exercise tests are technically VO2 peak because they don’t meet the testing criteria for being considered a true “VO2 max”. In these cases, a VO2 peak result usually still provides a reasonable approximation of CRF.
A quick interlude on METs
It took me a while to fully appreciate what metabolic equivalents of task (METs) are, and how they connect to VO2 max. It's worth understanding, because this pops up everywhere in fitness research.
One MET represents your body’s energy expenditure at rest. It’s roughly equivalent to:
- Burning 1 kcal per kilogram of body weight per hour
- Consuming 3.5 mL of oxygen per kilogram of body weight per minute
Your maximum METs is the ratio of energy you burn during your hardest possible exercise compared to your resting energy expenditure. So if your peak energy output is 10 times your resting energy output, that's 10 METs.
Because 1 MET equals roughly 3.5 mL O₂/kg/min, we can convert between METs and oxygen consumption (VO2) using the following formula:
VO₂ = METs × 3.5
And when applied to peak effort:
VO₂ max = Maximum METs × 3.5
This equation is how researchers and clinicians convert between the two units. Some studies report results in METs, others in VO2 max. When meta-analyses pull data from multiple studies, they typically convert everything into one format so they can be analyzed together.
One caveat on METs: the conversion of 1 MET = 1 kcal/kg/hour = 3.5 mL O₂/kg/min was originally derived from a single person: a 70 kg, 40-year-old man.2,3 More recent work shows that this relationship overestimates the energy expenditure and oxygen uptake at rest by about 10% in men and 15% in women.4 Despite these known shortcomings, the original equation is still the standard in the literature. Worth knowing, but not a deal-breaker for interpreting research.
In addition to providing a measure of CRF, METs also offer a way of describing the intensity of different physical activities relative to rest,5 expressed as multiples of 1 MET.4 The Adult Compendium of Physical Activities provides standardized MET values for hundreds of activities.6 Some examples:
- Lying or sitting: 1–1.5 METs
- Walking slowly: 2–3 METs
- Brisk walking or moderate biking: 3–6 METs
- Running, or biking faster than 16 km/h: 6+ METs
These standardized MET values can provide a starting point when describing exercise intensity. For example, anything with a value of 6 METs or higher is considered vigorous, 3–5.9 METs is moderate, and 1.6–2.9 METs is light. It’s important to keep in mind that these are averages — the same activity can require more or less METs for different people.
Why is CRF important?
The reason everyone — from cardiologists to health influencers — is so focused on CRF is simple: it's one of the strongest predictors of mortality we have. In fact, it’s even more predictive than traditional cardiovascular risk factors, like smoking, high blood pressure, and diabetes.7,8 The American Heart Association has issued multiple statements calling for CRF to be treated as a clinical vital sign.7,9
Large observational studies and meta-analyses consistently find that every 1 MET increase in CRF (about 3.5 mL/kg/min on a VO2 max scale) is linked to an 11–17% lower risk of dying.8,10,11 This pattern holds across sexes and age groups. The risk goes up sharply at the lower end of fitness, which means the people with the least fitness have the most to gain from improving.
What the Veterans study tells us
One of several landmark studies in this area followed more than 750,000 US Veterans and grouped them by where their CRF (in peak METs) fell compared to peers of the same age and sex.8 Here's how the categories shake out:
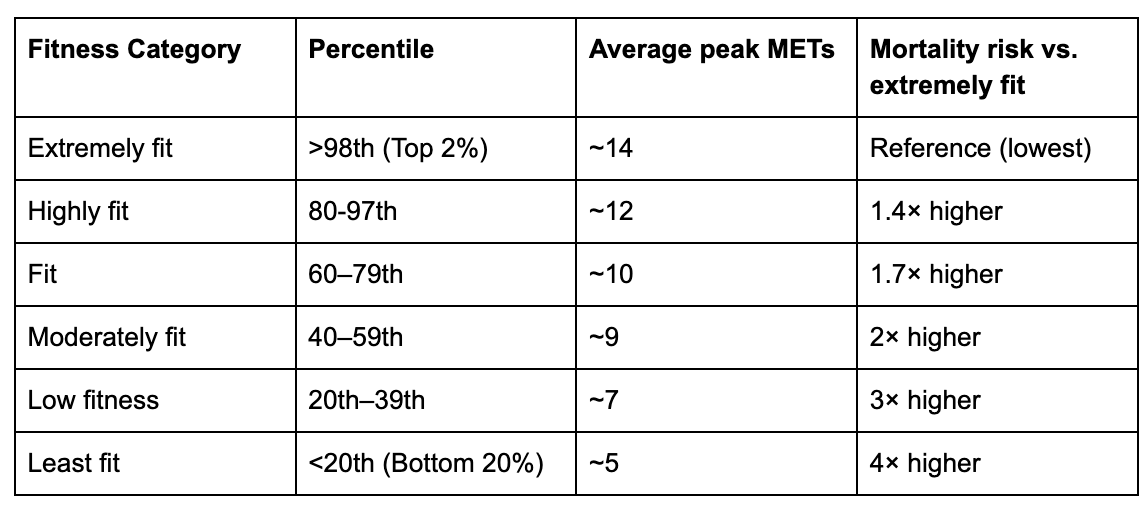
To put those MET values into context:
- 14 METs (extremely fit): running at around 15 km/h (4:00/km pace), cycling at ~300 watts or ~35 km/h on flat ground.
- 12 METs (highly fit): running at ~13 km/h, cycling at ~230 watts or 27 km/h, sustained high-intensity interval work like burpees and mountain climbers.
- 10 METs (moderately fit): running at ~10 km/h, cycling at ~175 watts or 24 km/h.
- 9 METs: running at ~9 km/h, cycling at ~150 watts or 22 km/h.
- 7 METs (low fitness): running at ~7 km/h, cycling at ~100–125 watts or 18 km/h.
- 5 METs (least fit): walking at 6 km/h on a treadmill, cycling at 60 watts or 14 km/h, mowing the lawn with a push mower, or shovelling snow at a moderate pace.
Other studies also point to 7.9 METs as a meaningful threshold — below this, the risk of death goes up significantly.1011
CRF predicts more than mortality
Low CRF isn't just about lifespan. It's also linked to higher risk of heart failure, stroke, type 2 diabetes, several cancers, dementia, anxiety, and depression.12 People with higher CRF tend to report better quality of life, miss less work, and spend less time in hospital.13,14
For athletes and active people, CRF is also a critical input for designing training plans and predicting performance.
The best part: CRF is changeable
Some of your CRF is genetic. But here's something interesting: genetically predicted VO2 max does not appear to be associated with mortality risk.15 This suggests that what you actually do — how active you are — matters more than the VO2 max predicted by your DNA.
If you don't exercise, your CRF naturally drops by about 10% per decade starting in your 40s, with a steeper drop after age 70.5 A consistent exercise habit can slow, halt, or even reverse that decline. People who are already very fit may aim to maintain their CRF, while people starting from a sedentary baseline can often gain 1–2 METs with a structured exercise program.16 This is significant: every 1 MET gain is linked to roughly a 15% reduction in mortality risk.17
Bottom line: Higher CRF is consistently linked to better health outcomes and lower mortality risk. And we can improve it through targeted exercise.
So if CRF is this important, how do we measure it?
How do we measure CRF?
Here's where things get messy. There are a lot of ways to figure out your CRF, and they vary a lot in accuracy.
- Direct measurement (the gold standard). A cardiopulmonary exercise test (CPET), done on a treadmill or stationary bike at maximum effort while wearing a mask that measures the air you breathe in and out. This is the only way to directly measure VO2 max.
- Maximal exercise tests without a mask. A structured treadmill or bike test where you push to exhaustion. Your peak workload–and sometimes other data–is plugged into a validated equation to estimate maximum METs (and, by extension, VO2 max).
- Submaximal exercise tests. A structured test (usually treadmill or bike) that stops before exhaustion. Your heart rate response and other factors are inputted into a validated equation to estimate max METs.
- Field tests. These include the 20-metre shuttle test, the timed 1.5-mile run, the 6-minute step test and the 6-minute walk test. Performance on the test is used to estimate VO2 max using prediction equations.
- Non-exercise prediction equations. Equations that estimate VO2 max from things like age, sex, weight, and self-reported activity. No exercise required.
- Wearables. Many wearables provide estimates of VO2 max. These are often based on heart rate and accelerometer data (how much and how fast you move), in conjunction with other parameters like age and sex. The exact algorithms used by most consumer wearable devices are proprietary, so we don't know precisely how they work.
The CPET is the gold standard — every other method is an estimate. So the next question is: how good are the estimates?
How accurate are the different ways of measuring CRF?
CPET. This is the most accurate option. One caveat: results from a cycle test are typically 5–20% lower than treadmill results for people who aren't trained cyclists. That's because non-cyclists often have to stop early due to leg fatigue before their heart and lungs are truly maxed out.18
Maximal exercise tests without a mask. Most prediction equations tend to overestimate VO2 max. The best-performing equations overestimate by around 5% on treadmill tests and 0.5% on cycle tests.19,20 The expected error depends on the testing protocol and equation used.
Submaximal exercise tests. These are less consistent, with typical errors in the range of 10–15%. They tend to underestimate VO2 max in young, athletic people, and overestimate it in older or less active people.21
Non-exercise prediction equations. A review of 28 of these equations found that most produced estimates that were statistically different from actual measured VO2 max. Only about half of the people tested were correctly classified into the right fitness category (high, medium, or low).22 These equations can be useful at the population level, but they're often off the mark for individuals.
Wearables. This is where things get even murkier. The evidence so far is limited and not particularly reassuring.
- Wearables tend to underestimate VO2 max in well-trained people, like endurance athletes, and overestimate VO2 max in untrained individuals, performing best in moderately trained people.23
- In terms of the magnitude of error, a 2022 review found that wearables that use exercise-based algorithms (including data collected during exercise) tended to underestimate VO2 peak, with 95% of errors ranging from −10 to +10 mL/kg/min. Wearables relying on resting estimates (no exercise data) fared worse, with 95% of errors ranging from −13 to +17 mL/kg/min.24
- Apple Watch has shown an average error of about 13%, with individual errors ranging from −6 to +18 mL/kg/min.25
- The Garmin fenix 6 has a lower average error of about 7%.26
Many things can introduce errors in wearable readings: the use of optical heart rate sensors (which can be less accurate, especially on darker skin tones), where you wear the device, your wrist anatomy, hydration, altitude, and temperature.
At NiaHealth, we looked at 107 of our users who had a directly measured VO2 max result from a CPET and a corresponding VO2 estimate from their wearable (most less than 2 days apart). Overall, our findings were similar to published research: wearables tended to underestimate measured VO2 max by an average of -3.89 mL/kg/min (a little more than 1 MET). The mean absolute percentage error was 14.99% (95% CI: 12.9 to 17.14%)--generally, this error should be less than 10% if results from a device are used for clinical purposes. When we looked at the difference between wearable-estimated VO2 max and CPET-measured VO2 max for individual NiaHealth users, 95% of them were within -19.42 and +11.63 mL/kg/min. In other words, if you use a wearable to estimate your VO2 max, you can be reasonably certain that your measured VO2 max would be no more than 19.4 mL/kg/min higher or 11.6 mL/kg/min lower than the estimated value–not a small range.
Bottom line: A formal CPET will give you the most accurate VO2 max. Maximal and submaximal exercise tests come close but tend to overestimate. Non-exercise equations and wearables are the least reliable for individual decision-making, though they may still capture trends over time.
Can we just use physical activity as a stand-in for CRF?
If higher CRF is linked to lower mortality, and exercise improves CRF, I wondered: can we skip measuring CRF altogether and just focus on how much we exercise?
The more active you are — especially at higher intensities — the lower your risk of dying. 27,28 And as with CRF, there doesn't seem to be a clear point where more activity becomes harmful.29,30 In the Framingham Heart cohort, increasing moderate-to-vigorous physical activity by just 17 minutes a day was linked to a 5% improvement in VO2 peak.31
But physical activity isn't a perfect substitute for CRF. A few things to know:
- Self-reported physical activity is associated with mortality, but it's a weaker predictor than CRF.32
- Accelerometer-measured activity (from a wearable or research-grade device) does predict mortality,27,28 but it correlates poorly with actual CRF — explaining only about 5% of the differences in fitness between people.33
- Even when you combine accelerometer data and self-reported moderate-to-vigorous physical activity, they together explain less than 11% of the variation in CRF between people. Age is a much stronger contributor.34
Bottom line: Physical activity matters for health and somewhat tracks with CRF, but it's not a substitute for measuring CRF directly.
So, how should I measure my CRF?
We've covered what CRF is, why it matters, how to measure it, and how accurate each method is. Now for the question that's been driving the recent online debate: what's the best way to actually measure your CRF?
CPET is the gold standard. We have strong evidence that directly measured VO2 max predicts mortality. But — and this is the key point — in more than 99% of studies linking CRF to mortality, CRF was estimated, not directly measured. (Note: this does not include wearable estimates. We don't yet have data linking those to mortality or hard health outcomes.)
So most of the data showing that CRF predicts mortality is based on estimated CRF, not measured VO2 max. Which raises a fair question: why pay for an expensive, uncomfortable CPET if a simpler test gives you similar information about where you stand?
A maximal or submaximal exercise test without a mask can give you a useful ballpark of your CRF, though you'll have some error. Non-exercise prediction equations are less accurate at the individual level, but still give you a directional sense. All of these methods show the same inverse relationship with mortality: higher estimated CRF, lower risk.
The case for getting a formal CPET is strongest if you:
- Want the most accurate number
- Plan to retest over time and track real changes
- Need precise heart rate zones for structured training or to support athletic performance
- Have a health condition where your clinician wants accurate CRF data
What about wearable estimates?
Wearable VO2 max estimates aren't validated in the way clinical tests are. The algorithms are proprietary, and the published evidence is limited. Some wearables produce errors comparable to validated estimation methods. Others are off by quite a bit.
It's also possible that wearable VO2 max estimates predict mortality and health outcomes — we just don't have the data yet. Additionally, new wearables are released faster than researchers can study them. For now, it’s recommended not to make clinical or performance decisions based on wearable-estimated VO2 max, and the American College of Cardiology suggests focusing on trends over time rather than absolute values when interpreting these estimates.35
Bottom line:
- For the most accurate number: get a CPET (VO2 max test).
- For a general sense of where you sit relative to peers and your mortality risk: a treadmill or cycle test without a mask is fine.
- Your wearable is a useful trend-tracker, but try not to fixate on the absolute number or get rattled by small fluctuations.
The bottom, bottom line: Whatever you choose, regular physical activity — especially moderate-to-vigorous intensity — is never the wrong move. You do not need a VO2 max number to start exercising more.
What did I decide?
As for my own little testing conundrum: I don't fully trust my Garmin's estimated VO2 max–based on published data for the fenix 6, I anticipate that my fenix 7 might be off by 7% or more. I can get a rough sense of my CRF from the MET demands of the activities I do regularly, or from a validated prediction equation. So, while I don't need a formal test to predict my longevity, if I want a precise picture — for setting my training zones, for tracking changes, and a little bit for bragging rights — a VO2 max test wouldn’t hurt.
I'll keep you posted on how I measure up.
Our research standards & process
At NiaHealth, we do not make decisions first and look for evidence later. The entire process — from which tests we offer, to how we interpret results, to the recommendations we make — is grounded in clinical evidence from the ground up. Our research team is continually reviewing the literature to make sure the information we provide reflects current medical evidence. And frankly, we don’t think “trust us” should be the standard here. We think you should be able to see the process for yourself. Learn more here.


