
Magnesium is an essential mineral involved in many critical processes in the body, including energy production, nerve and muscle function, and blood pressure regulation. We've included magnesium on all of our testing panels at NiaHealth since Day One, but we recently reviewed the evidence on this important nutrient — and that review led us to update our cutoffs. The research even convinced members of our own team to pay closer attention to their magnesium intake.
What is magnesium and why is it important?
Magnesium supports muscle movement, nerve function, heart rhythm, and energy production. It also helps regulate other important minerals, like calcium and potassium, and supports healthy bones, blood pressure, and metabolism [1]. Our bodies can't make magnesium, so we need to get it from food or supplements. More on those later.
When magnesium levels in the blood drop too low, people may experience:
- Muscle cramps, spasms, or twitches
- Generalized muscle weakness
- Fatigue or low energy
- Headaches or migraines
- Irregular heartbeat or palpitations
These symptoms can be linked to effects on the nervous system, muscles, and heart — particularly when magnesium levels are significantly reduced [1].
Low blood magnesium has also been linked to several health conditions, including high blood pressure, diabetes, heart disease, chronic kidney disease, and a higher risk of mortality [2].
How do you know if you're getting enough magnesium?
This is where things get interesting. Magnesium status is usually assessed using a blood test called serum magnesium. But less than 1% of the magnesium in our body is found in the blood. The rest is stored inside our cells. Bone is our body's largest magnesium reservoir, and when we aren't taking in enough magnesium, it gets pulled out of the bone to keep blood levels from dropping [1]. This means that blood levels of magnesium may be normal even when total body stores are low.
Another way to put it: if your serum magnesium level is below the lab reference range, you're almost certainly deficient — meaning that the body doesn’t have enough magnesium stored to maintain blood levels— but a “normal” magnesium level doesn't necessarily mean you're getting enough.
There are tests that better assess whole-body magnesium, but they typically involve an IV infusion of magnesium followed by a 24-hour urine collection — not pleasant or practical for most people. So we continue to rely on blood testing as the main way to check magnesium status.
Typical lab reference ranges for serum magnesium — including our previous NiaHealth range — sit around 0.65–1.05 mmol/L, though the exact range varies depending on the lab and the population being tested. The catch: a magnesium level at the low end of this range may still mean you aren't getting enough. This is called Chronic Latent Magnesium Deficiency, or CLMD.
Chronic latent magnesium deficiency
People with CLMD usually have blood magnesium levels in the low-normal range (around 0.65–0.85 mmol/L) and don't typically have any obvious symptoms — like cramps, tremor, weakness, seizures, or heart rhythm changes — since those tend to show up only when blood levels are clearly low. However, people with magnesium in this low-normal range have a higher risk of developing high blood pressure, diabetes, heart disease, and chronic kidney disease, and they may benefit from increasing their magnesium intake. Low magnesium can also trigger low-grade inflammation and oxidative stress [3].
What surprised us was this: using the traditional reference range (0.65–1.05 mmol/L), fewer than 1 in 10 people are flagged as having low magnesium. But when you use a cutoff of 0.85 mmol/L, that number jumps to more than 2 in 3 [4].
The updated NiaHealth magnesium reference range
In 2022, an international expert group recommended setting the lower cutoff for blood magnesium at 0.85 mmol/L [5]. The goal was to better identify people with CLMD, but this change has been adopted inconsistently across labs.
When we reviewed the evidence, we noticed something important. While there are no clinical trials showing that correcting CLMD directly improves hard health outcomes (like mortality or disease incidence), flagging a magnesium level below 0.85 mmol/L gives people an opportunity to look at their diet and consider eating more magnesium-rich foods. There's good evidence that a higher magnesium intake from food is linked to a lower risk of early death [6]. As an added bonus: increasing your dietary magnesium usually means eating more whole, unprocessed foods — which is great for overall health.
For people with a magnesium level below 0.85 mmol/L who can't get enough through diet alone, supplements are also an option. This is especially worth considering for people with conditions linked to low magnesium — such as high blood pressure, diabetes, or chronic kidney disease — or for people on medications that can lower magnesium, like diuretics and proton pump inhibitors [1].
Getting more magnesium from food
When it comes to building up your magnesium stores, food is the best place to start. People who get more magnesium from their diet have a lower risk of mortality — an effect that hasn't been seen with supplements alone [6].
Magnesium is found in many foods, with the highest amounts in nuts, seeds, legumes, whole grains, and dark leafy greens. Common sources of magnesium are shown in the box below.
Food sources of magnesium
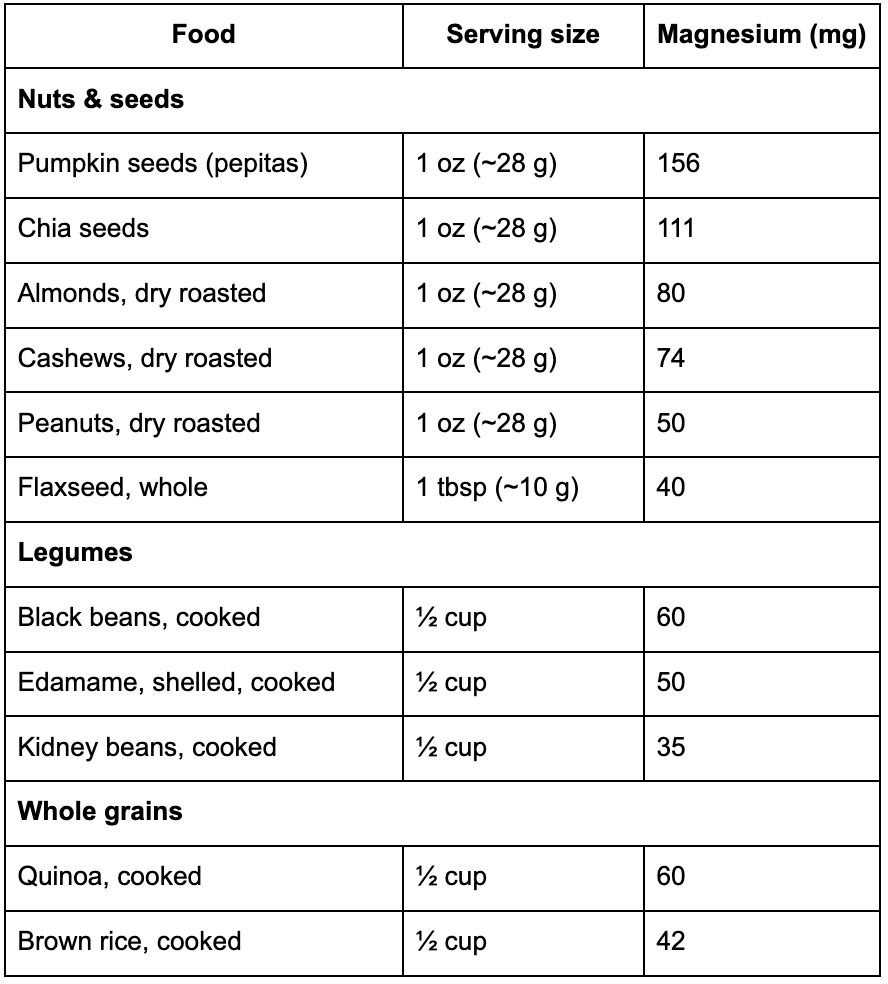
Reference: [7]
Current North American guidelines recommend 310–320 mg of magnesium per day for females and 400–420 mg per day for males. These numbers include magnesium from both food and supplements. US data shows that more than half of adults consume enough magnesium [8].
So if magnesium is in so many foods, why do so many people fall short? It turns out that average magnesium intake in North America has been dropping over time. This is partly due to changes in farming and partly due to shifts in what people eat. Western diets — which tend to be high in ultra-processed foods — usually have less magnesium, since up to 80% of the magnesium in food can be lost during processing. This is especially true for milled grains used in wheat and rice products [7]. For example, whole wheat flour contains about 120 mg of magnesium per 100 g, while refined flour contains only about 20 mg [7].
The takeaway: if you want to increase your magnesium intake from food, focus on plant-based whole foods with as little processing as possible.
Who should take a magnesium supplement?
Supplements may be helpful for people who:
- Can't get enough magnesium from their diet
- Have very magnesium levels below 0.65 mmol/L
- Have a condition where magnesium supplementation has been shown to help
The strongest reason to take a magnesium supplement is to correct an identified deficiency, or to prevent one in people with a known risk factor (such as long-term use of a proton pump inhibitor).
There's also solid research showing some additional benefits:
- Migraines: People who get frequent migraines have reported fewer episodes when taking magnesium supplements [9].
- High blood pressure: Magnesium has been shown to modestly lower blood pressure, especially in people with hypertension [10], [11].
Other potential benefits have been studied, with mixed results:
- Exercise recovery: Some — but not all — studies have shown that magnesium can reduce delayed-onset muscle soreness (the achiness that shows up a day or two after a hard workout), improve how recovered people feel, and lower markers of muscle damage [12].
- Exercise performance: Most studies have found that magnesium supplements don't improve athletic performance in people who already have enough magnesium [13]. However, magnesium deficiency does hurt performance in athletes, so correcting a deficiency makes sense, even if routine supplementation doesn't [14].
- Sleep: Some evidence suggests magnesium may improve sleep in people with insomnia, but the certainty is low because the studies have been small and have produced conflicting results. More research is needed [15], [16].
- Stress and anxiety: There's moderate-quality evidence that magnesium supplementation (300 mg/day) reduces stress in adults with magnesium levels of 0.85 mmol/L or below — particularly when combined with vitamin B12 [17].
- Muscle cramps: A 2020 systematic review found, with moderate certainty, that magnesium is unlikely to prevent cramps [18].
Which supplement is best?
There are many magnesium supplements on the market. The forms our bodies absorb best are organic salts, like glycinate, citrate, and L-Threonate. Inorganic salts of magnesium — chloride, carbonate, and oxide — aren't absorbed as well [1]. Generally, organic salts are preferred for this reason. Each of these have slightly different effects on the body:
- Magnesium glycinate is generally well tolerated and is a good choice if you want something gentle on the stomach.
- Magnesium citrate is more likely to have a laxative effect, which can be helpful for people who experience constipation.
- Magnesium L-Threonate is a newer form that may be better at raising magnesium levels in the brain, since it appears to cross the blood-brain barrier more easily.
As the most common side effect of magnesium supplementation is diarrhea, the effects of different formulations on the gut may be a strong factor in the decision of which one to take.
When it comes to dose, this depends on how well you tolerate the supplement and what you're using it for. Most studies show benefits at 200–400 mg/day. The official tolerable upper limit is set at 350 mg/day — based on diarrhea as the limiting side effect — but several studies have shown no significant problems at higher doses, up to 1,200 mg/day. People with significant kidney problems, however, usually need lower doses.
Some forms and doses are better suited to specific conditions:
- High blood pressure: Most studies showing a benefit on blood pressure have used magnesium citrate, oxide, or chloride at doses of 300–400 mg/day [11].
- Migraine prevention: The most-studied forms are magnesium citrate, dicitrate, and oxide, at doses of 400–600 mg/day (Department of Veterans Affairs and De...; von Luckner and Riederer 2018).
People taking a proton pump inhibitor who have low magnesium may also benefit from oral inulin, a type of prebiotic fiber [1].
To find the form and dose that works best for you, talk with your clinician about your goals.
Takeaways
- Most of us don't get enough magnesium. The recommended daily intake is 310–320 mg for women and 400–420 mg for men.
- Traditional cutoffs may miss people with low magnesium. A cutoff of 0.85 mmol/L may be more appropriate.
- If your magnesium level is below 0.85 mmol/L, use it as a chance to look at your diet — focus on whole, plant-based foods.
- People with magnesium below 0.65 mmol/L, or with conditions that increase the risk of low magnesium, should consider a supplement.
- Magnesium supplements may help prevent migraines and modestly lower blood pressure.
Our research standards & process
At NiaHealth, we do not make decisions first and look for evidence later. The entire process — from which tests we offer, to how we interpret results, to the recommendations we make — is grounded in clinical evidence from the ground up. Our research team is continually reviewing the literature to make sure the information we provide reflects current medical evidence. And frankly, we don’t think “trust us” should be the standard here. We think you should be able to see the process for yourself. Learn more here.


